

Hope is Not a Tactic.
It's time to stop acting like it is.

If your department’s heat illness prevention plan is “stay hydrated and let an officer know if you need a break,” you do not have a plan. You’re crossing your fingers and hoping.
We would never accept that kind of vagueness during accountability or rig checks. But when it comes to heat illness – one of the most predictable and preventable threats we face – we still tend to treat it like a personal problem instead of an operational hazard. We minimize rehab, and rely on firefighters to self-regulate when science clearly shows their decision-making is already being impaired. Then we act surprised when one of them becomes a patient or a statistic.
That is not a hypothetical concern. NIOSH has been documenting preventable firefighter deaths from heat illness for decades. In 2009, Cohnway Matthew Johnson collapsed during a 4.4-mile formation run in his first academy week. He was young, fit, medically cleared, and exercising in morning temps around 73 degrees. He still died of exertional heat stroke after a preventable chain of failures that included no hydration, inadequate cooling, and a conditioning program that ramped up too fast.
The same pattern shows up elsewhere. In 2019, Alabama firefighter candidate Jared Echols collapsed during an SCBA competence drill after having experienced heat illness in training the previous week. In 2012, Texas volunteer Captain Neal Wade Smith collapsed during a survival and entanglement course after showing early warning signs of disorientation.
None of them woke up thinking it would be their day.
Part of what makes heat illness so dangerous for us is how often it shows up as something easy to rationalize away: “I’m just tired.” “Just a headache.” “A little winded.” “Didn’t sleep much.” “A drama queen.” “Just dehydrated.” “Getting cranky.” “Probably anxiety.”
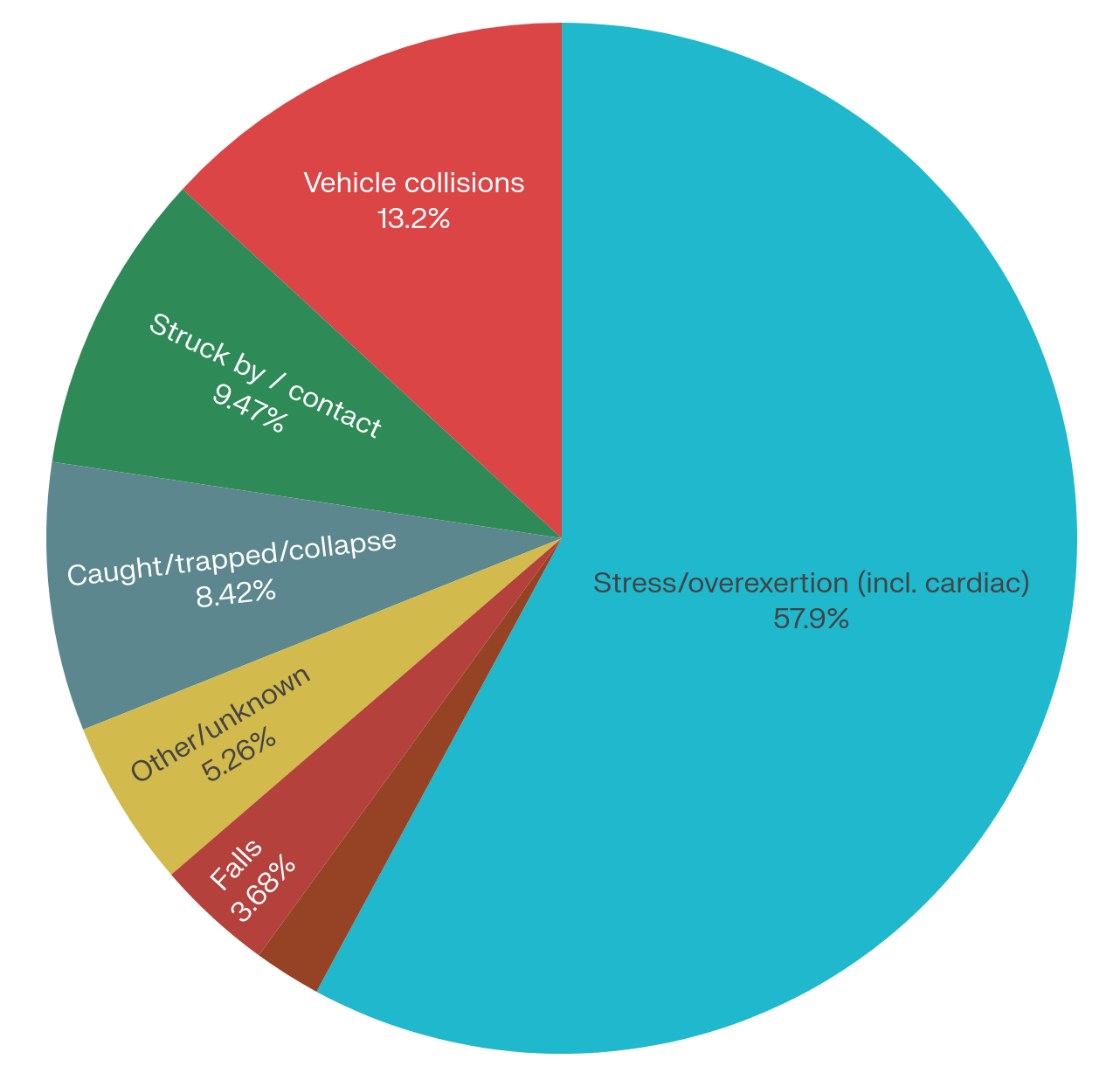
That cultural blind spot becomes clearer when you look at the data. We devote enormous time and energy to dramatic low-frequency hazards like maydays, collapses, and entrapments – and we should because these events, though rare, are catastrophic. But we under-prepare for the more predictable danger: our own physiology. The leading cause of firefighter injuries and line-of-duty deaths remains stress and overexertion by a wide margin. That category includes both heat illness and cardiac events, and the science shows more and more how the heat drives our cardiac risk.
Research on live-fire training has shown that firefighters’ core temperatures can stay elevated for hours afterward, while clotting risk rises and vascular function worsens. In other words, the heat and exertion we normalize on the job pushes the heart in dangerous ways. This is not about making the fireground softer. It is about recognizing the hazard and managing it intentionally.
That starts with understanding what makes firefighters so vulnerable to heat strain in the first place. Heat generated by working muscles that normally vents off, gets trapped by our turnout gear and SCBA. Sweat becomes less effective. Core temperature quickly rises. Central nervous system function drops and decision-making gets worse before many firefighters realize they are in trouble. Add back-to-back evolutions, short staffing, sleep debt, dehydration, stimulants like caffeine and nicotine, and a culture that glorifies “the grind” while treating rest as a deadly sin… now you’ve got a system primed for failure.
And that is exactly why heat illness cannot be treated as a self-report problem. The same rising core temperature that puts firefighters at risk also degrades the judgment needed to recognize and report it.
Recognition has to be simple, operational, and part of our training. There are different levels of heat illness, but the hard-and-fast rule should be straightforward: if a working firefighter has altered mental status – confusion, clumsiness, irrational behavior, slurred speech, momentary blackouts, or a collapse – that is heat stroke until proven otherwise, and a life-threatening emergency.
The trouble is we have a habit of explaining away early warning signs instead of acting on them. We tell ourselves we can’t spare anybody right now. We promise we’ll deal with it after this bottle, after overhaul, after this rep. That is how a manageable physiology problem turns into a rescue problem.
We need to stop rewarding the wrong hero.
We still praise the firefighter who worked the whole job without rehab, and we treat early reporting like weakness. But the firefighter who speaks up early, the officer who pulls someone before they crash, and the crew that treats rehab as part of the operation instead of a punishment – that is what strong leadership actually looks like.
Rehab is tactical.
And if rehab is tactical, it cannot depend on whether a firefighter is willing to admit they need a break in front of their peers. It needs to be built into operational plans with defined triggers, trained officers, active cooling capability, and a written SOG that removes guesswork. That means deciding in advance when crews automatically go through rehab – after live fire, after prolonged operations, after a set amount of bottle or PPE time – and who is responsible for enforcing and tracking it. It also means defining what symptoms trigger escalation and what the automatic response will be for heat cramps, altered mental status, or collapse.
This is also where the standards and regulatory picture matter. OSHA has been moving toward a formal Heat Injury and Illness Prevention rule for workplaces, using heat triggers, written plans, training, and response requirements. The final boundaries for emergency response are still unsettled, and the fire service may not be covered in the same way as other industries. But the direction is obvious, and uncertainty is not a reason to wait. NFPA 1580 lays the groundwork: departments should already have defined rehab processes, cooling options, monitoring, accountability, and return-to-duty criteria.

In other words, this is not some future problem to figure out later. Leading departments are building these systems now.
A workable heat illness SOG does not have to be fancy. It does have to be clear. The real work, though, is leadership and culture. Officers have to model behaviors, enforce triggers, and drive home the message that time in rehab is not tapping out. It’s doing the job in a way that keeps crews effective, keeps operations moving, and keeps firefighters going home. If your department needs a “starter” heat illness SOG, I’m happy to share one – feel free to reach out.
Heat illness is not a surprise; it’s a predictable operational hazard. Departments that fail to define clear triggers and rehab practices, train on them, and build enforceable SOGs around them are not managing risk – they are gambling.
Hope is not a tactic. It is time to stop acting like it is.
I appreciate this information and also the comment that "rehab is not tapping out". Thank you for spreading this message. My husband was a fire captain in Vancouver, BC and passed away from occupational cancer in August of 2024. In Canada, cancer is the #1 cause of death for firefighters (85%!), and it is 66% in the USA. I am writing a book (a memoir) on our story in honour of my husband that will include the subtle unravelling of our love story due to undiagnosed PTSD, which I believe contributed to his cancer. I am also trying to spread the word about "lifestyle leadership". I am writing my book for firefighter spouses and firefighters. Glad to have come across your Substack. Keep up the good fight, Roy.